The collection of medical doctrine supports governing the planning of Canadian Forces Health Services on operations at home or abroad, within the framework of either a single service, joint, multinational, or multinational joint task force.



Other International Fora: a collection of doctrine-related publications from other international organizations



About Us
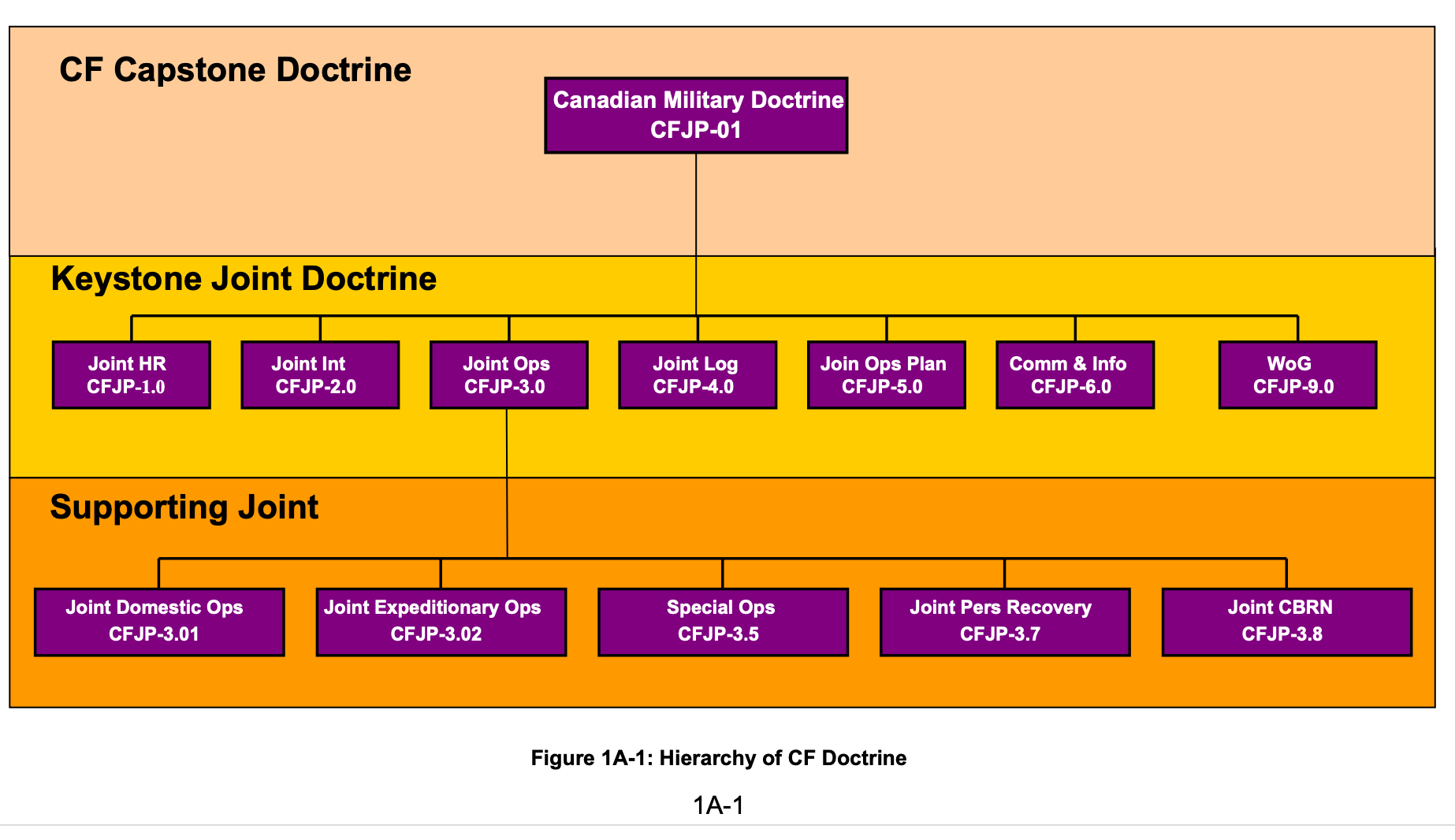
Doctrine is defined as, fundamental principles by which military forces guide their actions in support of objectives. It is authoritative but requires judgment in application. It embraces established wisdom in the areas of problem solving, decision making and planning, and is sometimes defined as simply “what is taught.”
Interoperability is achieved when Allies act together coherently, effectively and efficiently to achieve tactical, operational and strategic objectives. It reduces duplication and enables pooling of resources, producing synergies between nations’ forces.
The Directorate Health Services (HS) Strategy Doctrine and Interoperability Section is responsible for developing and managing HS doctrine that supports CAF operations at home or abroad, within the framework of either a single service, joint, multinational, or multinational joint task force.

The Directorate Health Services (HS) Strategy Doctrine and Interoperability Section is actively engaged in several key activities:
Frequently Asked Questions






Roles of Medical Support
“A category that identifies the functions and capability of a medical unit or element. Medical care is categorized into four roles. Most of the care capabilities of each role are intrinsic to the next higher role."" To be consistent with NATO, Canada uses the term medical rather than health services when describing Roles. In this case medical includes dental.
- Roles of medical support are not tied to levels of command. Rather, the term “role” is based on the clinical functions it provides.
- Likewise, roles of medical care do not equate to levels of sustainment or lines of support which are described in B-GL-300-004/FP-001
- A certain role of medical support does not imply a particular size or location in the battlespace.
Roles of medical support may be co-located. For example, during a counter-insurgency operation a Forward Surgical Team (a subset of Role 2) may be co-located with a UMS (a subset of Role 1) at a battalion-sized forward operating base.

The flow of casualties and acute medical cases usually follows a linear continuum of care; however, as depicted in Figure 1-1, one or more roles of medical support may be bypassed due to patients’ needs, the proximity, workload and capacity of MTFs, and the en route care capabilities of the MEDEVAC team.
The First Response Capability: Point-of-Injury Care
Although not a doctrinal role of medical care, the first response capability is listed in this section to emphasize its importance for the outcome of clinical treatment and to showcase where the continuum of care begins. Clinical outcomes are influenced by those who apply the first field dressing
Point-of-injury care. The aim of the care given at the POI is to remove the casualty from immediate threat and to avoid further deterioration of vital functions through immediate lifesaving measures.
- Whenever practicable, first aid for the most seriously injured should take place immediately, but not longer than within 10 minutes of injury.
- Often this is conducted by non-medical personnel trained to deliver combat first aid or tactical combat casualty care (TCCC).
- Security is the foundation of safe and effective care. Before rushing to treat casualties, effective enemy action must be suppressed.
- The best medicine on the battlefield is to win the firefight.

Role 1 Medical Support – Emergency and Primary Health Care
Role 1 medical support, “Provides routine primary health care, specialized first aid, triage, resuscitation, and stabilization.” Role 1 medical support provides:
- advice to the chain of command on basic occupational and preventive health issues;
- routine, daily sick parade and the management of minor sick and injured personnel for immediate return to duty;
- a minimal patient holding capacity; and
- preparation of patients for evacuation to the next appropriate higher-level treatment.
Unless enhanced by a surgical capability, a Fd Amb provides only Role 1 medical support. Examples of Role 1 MTFs are the UMS, the BMS, and the airfield medical station.

Role 2 Medical Support – Surgical Care Capability
Role 2 medical support, “Provides a capability for the reception and triage of casualties, as well as the structure to perform treatment of wounded, injured and diseased at a higher technical level than Role 1, including resuscitation and surgery.
Role 2 MTFs capabilities routinely include emergency intake, DCS, diagnostics, a post-operative capability, medical supply, C2, and a limited holding facility for the short-term holding of casualties until they can be returned to duty or evacuated. There are three types of Role 2 MTFs - , and
- Forward Surgical Team (FST);
- Role 2 Basic (Role 2B); and
- Role 2 Enhanced (Role 2E).


Role 3 Medical Support - Deployed Hospital Care Capability
Role 3 medical support, “Provides the structure for deployed hospitalization with the elements required to support it, including a mission-tailored variety of clinical specialties and support functions. Dental capabilities comprise comprehensive dental care and oro-maxillofacial surgical capability. Patients who cannot be returned to duty in accordance with the theatre patient return policy are evacuated out of theatre.
A Role 3 MTF must provide all the capabilities of the Role 2E MTF and be able to conduct specialized surgery, specialized care, computed tomography, oxygen production and additional services such as neurosurgery and internal medicine as dictated by mission and theatre requirements.

Role 4 Medical Support - Full Spectrum Hospital Care Capability
Role 4 medical support, “Provides the full spectrum of definitive medical care that cannot be deployed in the theatre or is too time-consuming to be conducted there. Role 4 includes highly specialized medical procedures, specialist and reconstructive surgery, and rehabilitation. It is normally provided in Canadian civilian facilities.


—E.M. Earle
Makers of Modern Strategy & 1944
The highest type of strategy—sometimes called grand strategy—is that which so integrates the policies and armaments of the nation that resort to war is either unnecessary or undertaken with the maximum chance of victory.

—Napoleon I,
Maxims of War, 1831
War should be made methodically, for it should have a definite object; and it should be conducted according to the principles and rules of the art.

Karl von Clausewitz
On War, 1832
War is not only chameleon-like in character, because it changes its colours in some degree in each particular case, but it is also, as a whole, in relation to the predominant tendencies that are in it, a wonderful trinity, composed of the original violence of its elements, hatred and animosity, which may be looked upon as blind instinct; of the play and probabilities and chance, which make it a free activity of the soul; and of the subordinate nature of a political instrument, by which it belongs purely to reason.
B.H. Liddel-Hart
Strategy, 1954
The true aim is not so much to seek battle as to seek a strategic situation so advantageous that if it does not of itself produce the decision, its continuation by a battle is sure to attain this.

Aristotle
Ancient Greek philosopher (384–322 BC)
“We are defined by what we do repeatedly, therefore excellence is a habit, not an act.”







Contact Us
Get in touch
Location:
60 Moodie Dr, Nepean, ON K1A 0K2
Call:
+ 1 613-901-8242